By A Mystery Man Writer

Breast Cancer Breast cancer is the second leading cause of cancer deaths in most US populations (it's number 1 among Hispanics); it is the most commonly diagnosed cancer worldwide. 1% of breast cancers occurs in men, who are often diagnosed at later
Breast Cancer Breast cancer is the second leading cause of cancer deaths in most US populations (it's number 1 among Hispanics); it is the most commonly diagnosed cancer worldwide. 1% of breast cancers occurs in men, who are often diagnosed at later stages. Risk Factors Include: Age; most breast cancers are diagnosed in women over 50 years old. Family history; women with 1st degree relatives (mothers, daughters, sisters) with breast cancer are 2-3 times more likely to develop breast cancer than women without family history. Genetics; women with mutations in BRCA1 or BRCA2 genes have a 70% chance of developing breast cancer by age 80. These genes are also associated with higher risk of ovarian cancer. Thus, we screen for mutations in these genes in women with 2 or more relatives with breast cancer. Men with BRCA mutations have a 1-2% lifetime risk of developing breast cancer. Higher lifetime estrogen exposure; this includes early menarche, late menopause, and late first pregnancy. History of non-cancerous breast lesions; benign lesions associated with slight increase in risk include fibroadenoma, hyperplasia, sclerosing adenosis, papilloma. Synthetic estrogens; women who are taking hormonal contraceptives or hormone replacement therapy in menopause have a slightly increased risk of developing breast cancer; it is notable, however, that hormonal contraceptives have protective effects against ovarian and other types of cancer. Radiation therapy; women who have been exposed to radiation therapy for other cancers have an increased risk for breast cancer. Lifestyle factors; dietary habits, cigarette smoking, elevated alcohol intake, and low rates of physical activity also contribute to the risk of breast cancer. Screening & Diagnosis: Fortunately, breast cancer screening programs have greatly reduced breast cancer mortality rates in wealthy countries. Recommendations for mammograms have varied over the years and by age group, but the National Comprehensive Cancer Network currently (as of 2022) recommends that all women with average risk of breast cancer should start receiving annual mammograms at age 40. Those with higher-than-average risk should start their annual mammograms earlier, and have physical exams every 6-12 months. Some sources also recommend that higher-risk patients have regular MRIs performed. Malignant lesions on mammogram: hypoechogenicity internal calcifications, shadowing, spiculated, indistinct, angular margins. Biopsies and ultrasound help us to distinguish malignant vs nonmalignant lesions. Metastatic cancer: Most common sites are bone, liver, lungs. Treatments: For breast cancers range from breast-conserving treatments to full mastectomy; in some patients, radiation may also be recommended, and, in some cancers, targeted treatments are effective. We'll come back to this, later. Breast Changes in Cancer Pain and/or changes in the size or shape of the breast New lumps in the breast or axillary region. Nipple inversion, shrinkage, pain, or bloody or mucus discharge. Swelling or redness of the breast or thickening, dimpling, or flaking of the skin of the breast. Changes to the nipple and skin of the breast are sometimes described as having an "orange skin" or "peau d'orange" appearance. Epithelial Breast Cancer Most breast cancers arise in the epithelia of the lobules or ducts. Receptor Type: One of the steps in diagnosing breast cancer is determination of diagnosing breast cancer is determination of which, if any, receptors the cancer cells express: Estrogen and progesterone receptors, and HER2 (human epidermal growth factor receptor 2). This helps us determine which targeted therapies will be most effective. When a patient is negative for all three receptors, we call this Triple Negative cancer. Immunophenotype: ER and PR are expressed in ~75% of breast cancer cases. ER/PR-positive cancers are usually low grade, less aggressive. Some cancers are positive for only ER or PR; these seem to be more aggressive, less responsive to hormone therapy. ~15% of breast cancers overexpress HER2; these cancers have a more aggressive clinical course with poor prognosis; they are responsive to anit-HER2 therapy. 10-15% are triple-negative – poor prognosis, do not benefit from current targeted therapies. Molecular subtypes: Luminal A – HR+/HER2- (most common in US) Luminal B- HR+/HER2+ Triple negative HER2+ Normal-like breast cancer In situ vs Invasive carcinoma: Normal: A simplified, normal duct or lobule represented by a ring of epithelial cells. Carcinoma in situ: cellular hyperplasia crowding the lumen of the duct or lobule. Invasive carcinoma: the cancer cells breach the basement membrane of the duct or lobule, and spread to surrounding tissues. Ductal carcinoma: Ductal Carcinoma In Situ is a highly heterogenous group of lesions. Calcifications on mammograms are a key indicator of ductal carcinoma, but be aware that calcifications are not exclusive to carcinoma. Ductal carcinoma in situ is a precursor lesion for invasive ductal carcinoma, so we remove any tumors we find. Ductal carcinoma in situ: Invasive ductal carcinoma is the most common form of invasive breast cancer, accounting for approximately 75% of all cases. Histologically, most of these are of "no specific type" (NST) – but be aware of rarer subtypes of invasive ductal carcinoma, including medullary, tubular, papillary, and mucinous. Invasive ductal carcinoma: Lobular carcinomas Reduced e-cadherin expression is a clue that the patient has lobular carcinoma. The loss of e-cadherin accounts for the loss of normal lobule architecture in these lesions. Lobular Carcinoma In situ, aka, lobular neoplasia, is not cancerous, nor is it a precursor lesion for invasive lobular carcinoma (some authors disagree with this, and consider LCIS to be a precursor lesion, based on studies that show a stronger relationship between LCIS and invasive carcinoma than previously found). Lobular carcinoma in situ: Lobular carcinoma in situ is associated with an increased risk of breast cancer overall, and thus warrants close observation. Treatment varies by patient; in some cases, monitoring for new changes in the breast may be sufficient, but others may require chemotherapy or surgical removal. In most cases, lobular carcinoma in situ is found incidentally, when the breast has been biopsied for a nearby lesion; most patients do not have indicative lumps or calcifications, as seen in other breast cancers. Invasive lobular carcinoma The second most common invasive breast cancer, accounting for approximately 10% of all cases. It is typically found during mammogram screenings or when patients present with the changes in breast tissue described earlier. Invasive lobular carcinoma: Inflammatory Breast Cancer: Very rare, accounting for only 1-5% of breast cancers, but is aggressive. Lesions may be found in the ducts or lobules, and occur when cancer cells, usually from invasive ductal carcinoma, block the lymph vessels. Patients present with rapid onset of erythema and edema over a large area of the breast. Paget Disease of the Breast: Characterized by eczema-like changes to the skin of the nipple/areola. When patients present with this, we need to test for ductal carcinoma (which may be in situ or invasive). For references, see full tutorial.

19. Breast pathology Flashcards

Mammography Flashcards iPhone and iPad medical app review

Ditki, Medical & Biological Sciences - Our newest tutorials address benign and cancerous breast lesions - coming soon! www.drawittoknowit.com #ditki #usmle #meded #medschool #medstudent #highered #breastcancer #pathology #benignbreastdisease #nursing
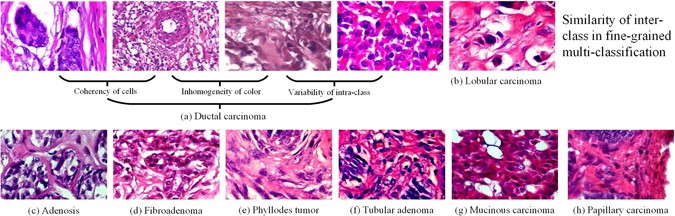
Breast Cancer Multi-classification from Histopathological Images with Structured Deep Learning Model

11/19- Breast Pathology Flashcards by Kathryn Kudlaty

Pathophysiology of disease flash cards by Carlos Gonzalez - Issuu

Free Medical Flashcards, 2500+ Free Flashcards

Breast Pathology Flashcards

Breast Pathology PATHOMA 2 Benign Conditions + Risk Factors of Breast Cancer

Treatment of Breast Disease Flashcards by Brian Mendonsa

Breast cancer: Video, Anatomy, Definition & Function
Internal Medicine Board Review - Oncology Flashcards - by Knowmedge

Pathology of breast: benign lesions Flashcards

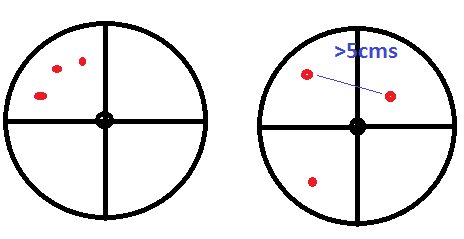
Breast Cancer T Staging: A Visual Guide
Breast Pathology II